Přejít k obsahu
|
Přejít k hlavnímu menu
Menu
Registr
Vstup do registru
Výstupy z registru
Technologie registru
Kontakt
Zápisy
Doporučení
Doporučení ČR
Doporučení - mezinárodní
Doporučení - archiv
Aktuality
Síť center
Pro pacienty
Pro dospělé
Pro děti
english
Výstupy z registru ČNHP za rok 2025: hemofilie
This slide describes the process of records‘ validation within the registry. All patients have signed IC.
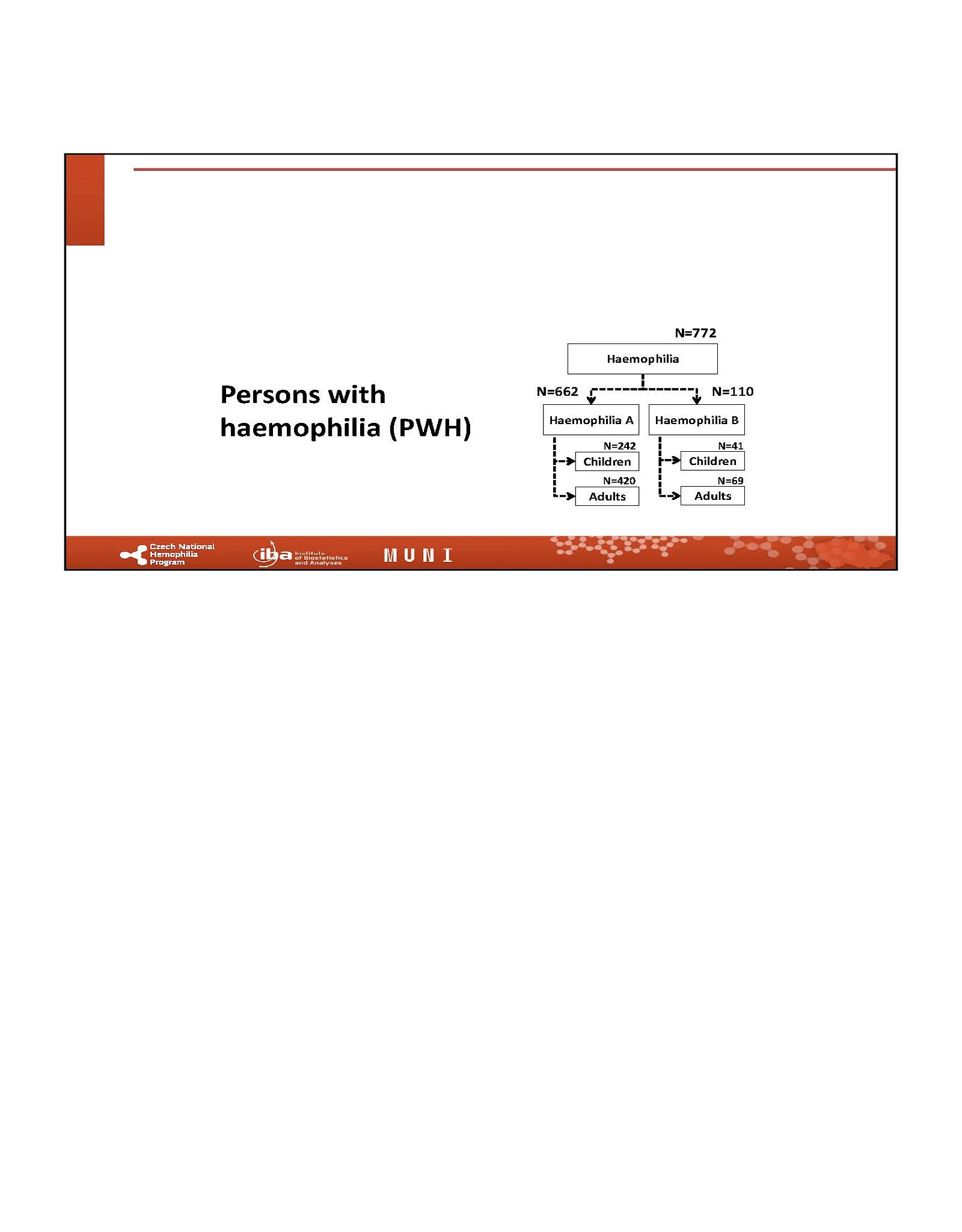
Centres contributing to the CNHP registry.
Though the percentage of PWH over 65 years has not been increasing dramatically over last several years, dealing with elderly people with haemophilia will be the challenge for treaters. Currently it counts over 11% of all registered PWHs.
Summary description of the PWH with inhibitors within registry. Number of PWHI is same as in 2024. Two new inhibitors developer and 2 disappeared while on emi (this does not necessarily mean, that those patients are tolerant to FVIII, though).
This slide describes in more details all PWH with “active” inhibitors within CNHP registry. No patient is on ITI. All HA inhibitor patients are now on emicizumab prophylaxis. The number of bleeds, on above mentioned treatment is kept low.
All patients with inhibitors, are on permanent prophylaxis. This treatment led to minimal ABR in all HA inhibitor patients.
Median age at diagnosis differs between adults and children with HA, mainly due to improved diagnostics over time. Today, most children with severe haemophilia are diagnosed before 12 months of age, steadily reducing the average diagnostic age each year.
Mean age of Czech adults with HA is over 40 years. Mean age of children with HA is around 10 years.
No HepC infection in children since late 90’s. None of Czech children with HA is infected with Hepatitis C.
There was NO NEW HepC infection in 2025. Number of HepC RNA positive persons is decreasing on antiviral therapy
No HIV positive PWH. No new HIV+ PWH reported since late 90s.
No HIV positive PWH. No new HIV+ PWH reported since late 90s.
Czech PWH show good care overall, with median ABR 0 in severe HA since 2021 (children 0.4/0, adults 1.0/0; vs. 2024: 0.8/0 and 0.9/0). However, in moderate HA children, median ABR rose from 0 to 1, suggesting less optimal control than in severe HA.
There was no CNS bleed in children with haemophilia in 2025. Percentage of children with bleed was higher, than in 2024 (22,8%), but lower, than in 2023 (29,6%)
Bleeding events and number of “non-bleeders” in adults was similar to 2024.
This figure refers to preventive factor’s administration in children with HA There was significant decrease in this parameter compared to 2024.
This figure refers to preventive treatment in adults with HA.
Prophylaxis in children with severe HA remains highly effective, with median ABR at 0. However, bleeds in moderate HA increased vs. 2024.
Prophylaxis is highly effective in Czech adults with severe HA, maintaining median ABR and joint ABR at 0. However, some patients still experience significant joint bleeding despite prophylaxis.
Lower bleeding rates are seen in PWH born after 1990. However, median ABR in severe HA on prophylaxis remains 0 in both groups, supporting its benefit even with existing joint damage.
Joint bleeds show a similar pattern in adults, with some frequent bleeders remaining, especially in those born before 1990, who may need intensified or tertiary prophylaxis.
Only below 30% of bleeds in children with haemophilia are joint bleeds. Soft tissue bleeds are in 34% subcutaneous bleeds. The most of all bleeds in children are traumatic bleeds.
Median treatment for joint bleeds in children was 2000 IU FVIII (1 infusion), and 3000 IU for muscle bleeds. Some bleeds resolved without extra dosing, on prophylaxis alone.
In adults, most bleeds are joint (57%) or muscle (53%), with 70% of joint bleeds being spontaneous, likely due to pre-existing joint damage, especially in those born before 1990.
Median treatment for joint bleeds in children was 2000 IU FVIII (1 infusion) and 3000 IU for muscle bleeds. Some bleeds resolved without additional dosing, on prophylaxis alone.
Across paediatric centres, median ABR in severe HA on prophylaxis is ≤1/year. Further individualized prophylaxis may help reduce inter-centre differences and improve outcomes, including in moderate HA.
In 2025 the difference in ABR of adults with severe HA on prophylaxis is negligible between centres. Vast majority of adult PWHs with severe disease on permanent prophylaxis had median 0 bleeds.
Goal of prophylaxis is equal or lower bleeding than without it. Patients who bleed need prophylaxis; those with very low bleed rates may not. Care should reflect active lifestyles in children.
Similar information for adults.
More detailed description of prophylactic dosing/regimens used by different paediatric centres within CNHP and its correlation with annual bleeding rates in respective centres.
More detailed description of prophylactic dosing/regimens used by different adult centres within CNHP and its correlation with annual bleeding rates in respective centres.
Children on prophylaxis in 2025 are in 99% on permanent prophy.
Similar slide for adults
This slide describe the population of HA patients treated with emicizumab in CZ. It is seen, that emi is used mainly for people with HA without inhibitors and its efficacy is very high for both children and adults.
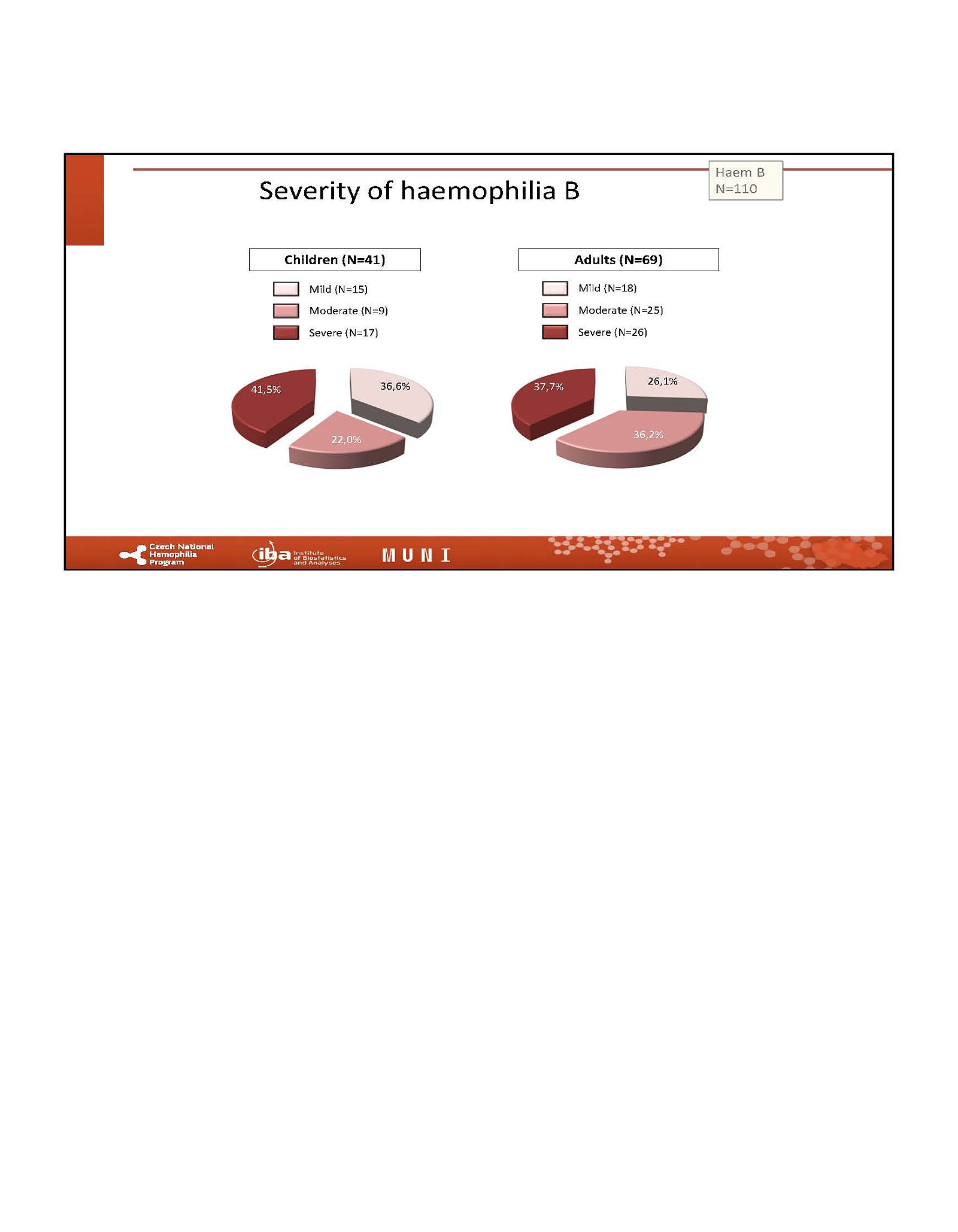
There is no major difference in demographics between HA and HB.
There is no major difference in demographics between HA and HB.
NO HepC infection in children since late 90’s. None of Czech children with HB is infected with Hepatitis C.
There was NO NEW HepC infection in 2024
Very low number of HIV positive PWH due to low/no access to contaminated concentrates in 80s and 90s. No new HIV reported in any PWH since late 90s.
See previous comment for the same slide related to HA.
Data shown document good efficacy of care provided to Czech PWH, no matter what age category they are. Mean/Median numbers of bleedings per year (ABR) are similar to 2024, only median for children with severe HAB increased to 1.
There was no CNS bleed in children with haemophilia B in 2025. 63,4% of children had no bleed at all. Was 66.7% in 2024. More bleeds required hospitalisation (from 4 to 7)
Bleeding events in adults. 70,6% HB adults with no bleed (similar to 2024). Less bleeds required hospitalisation (from 9 to 3)
This figure refers to preventive factors administration in children with HB.
This figure refers to preventive factor administration in adults with HB.
The data on bleeding rate in children with HB. Median ABR in children with severe haemophilia B increased for both on prophylaxis and on demand compared to 2024, Thus it was higher, than in HA.
As well as in HA, adults with severe haemophilia B, who bleed frequently should be commenced on prophylaxis. No major change compared to 2024.
Description of the type and localisation of the bleeds in children with HB.
Joint bleeds in children were treated with median dose of 4000 IU FIX administered in 3 infusions in four days. Muscle bleeds in 3 children needed median dose of 2000 IU FIX in 2 infusions over 2 days.
No major difference between HA and HB bleeding. Most of bleeds are spontaneous joint bleeds, most frequently elbow.
In adults, muscle bleeds are treated with 4000 IU FIX in total, administered in two infusion over 2 days in most of the cases. Joint bleeds needed 10500 IU mostly in one infusion (large interwal, though).
Not all centres treat children with HB. The median ABR is still slightly higher than for HA. Though this is, indeed, due to small total numbers.
Similar situation for adults with HB, but apart from one patient, the ABR is similar to HA.
This slide describes the treatment of children with HB regardless of prophylaxis in those centres, which treat PWHB.
This slide describes the treatment of adults with HB regardless of prophylaxis in those centres, which treat PWHB.
More detailed description of prophylactic dosing/regimens used by different paediatric centres within CNHP and its correlation with annual bleeding rates in respective centres. All children with HB are treated with EHL FIX in 2025.
More detailed description of prophylactic dosing/regimens used by different adult centres within CNHP and its correlation with annual bleeding rates in respective centres. EHL FIX is dominating also in adults.
More children on prophylaxis in 2025 compared to 2024. Most of them on permanent prophy.
No major change compared to 2024. All of those, who are on prophylaxis are on permanent one in 2025
Most PWH are now treated with EHL concentrates. Only 11 use plasma-derived products. Emicizumab use increased to 89 patients in 2024, with some patients switching products during the year.
Only one child in the CNHP registry used a plasma-derived concentrate in 2025. Most were switched to EHL (mainly Elocta or Altuvoct), and emicizumab use is increasing, especially in children.
Only 10 adults registered in CNHP registry were treated still with plasma derived concentrates in 2025 (was 16 in 2024). The number of adults treated with recombinants is further increasing over last years with most of them being treated with EHLs.
This table compares data between 2024 and 2025. E.g. you can see, that percentage of patients treated with recombinant EHL concentrates and registered within CNHP registry changed from 65,2% in 2024 to 75,1% in 2025.
Similar slide for children only.
Similar slide for adults only.
This slide describes in graphical form the changes of treatment used during last 12 years in CZ. Switch from pdF to SHL rFVIII and EHL rF is clearly seen as well as the continuous boom of emicizumab.
Trends are even more clearly demonstrated in children.
Same information for adults.
Data reflect CNHP registry records updated in 2025. The key metric is average annual consumption per treated person, representing nationwide factor use per PWH by concentrate type.
CNHP 2025 data show average annual factor use per treated person. SHL dosing is similar across ages, while EHLs vary by weight and appear appropriate; adults on SHLs may still be underdosed.
CNHP 2025 registry data show average annual factor consumption per treated PWH as the key national metric.



.")









. However, in moderate HA children, median ABR rose from 0 to 1, suggesting less optimal control than in severe HA.")
, but lower, than in 2023 (29,6%)")








, and 3000 IU for muscle bleeds. Some bleeds resolved without extra dosing, on prophylaxis alone.")
 or muscle (53%), with 70% of joint bleeds being spontaneous, likely due to pre-existing joint damage, especially in those born before 1990.")
 and 3000 IU for muscle bleeds. Some bleeds resolved without additional dosing, on prophylaxis alone.")
















 are similar to 2024, only median for children with severe HAB increased to 1.")
")
. Less bleeds required hospitalisation (from 9 to 3)")







.")









, and emicizumab use is increasing, especially in children.")
. The number of adults treated with recombinants is further increasing over last years with most of them being treated with EHLs.")








